![]()
日本語
English
![]()
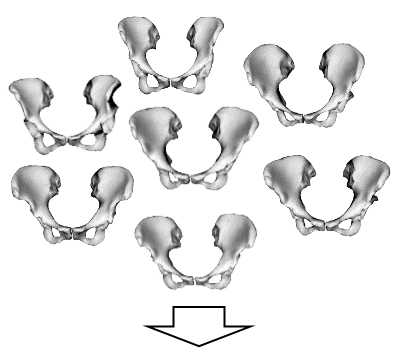
A statistical shape model is a model that performs statistical analysis (e.g., principal component analysis) on medical image data (e.g., CT) of many patients taken in the past to represent various organ shapes that differ from patient to patient with an average shape and a few deformation component (principal component) parameters. This allows complex organ geometries (e.g. pelvis) to be represented with only a small number of variables (e.g. 10-30). We are using this model to study algorithms for more accurate and stable image segmentation and disease progression analysis.
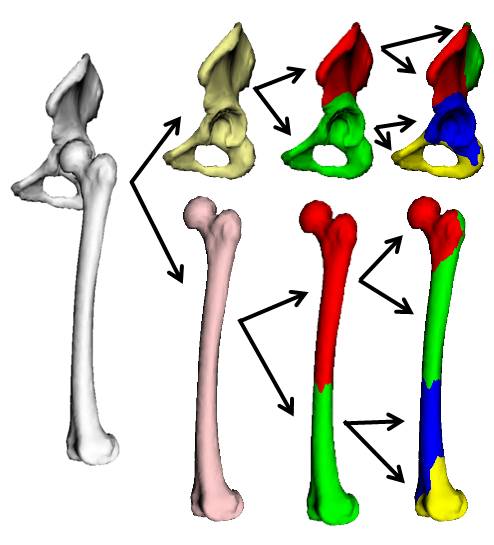
Statistical shape models have the advantage of being able to represent a wide variety of shapes with a small number of parameters, but they have the problem of having a large error margin when there are parts of an organ with a large amount of variation between patients and parts with a small amount of variation. To address this problem, we are studying hierarchical statistical models that consider one or more organs of the human body as a hierarchical structure consisting of multiple submeshes, and construct a statistical model for each submesh.
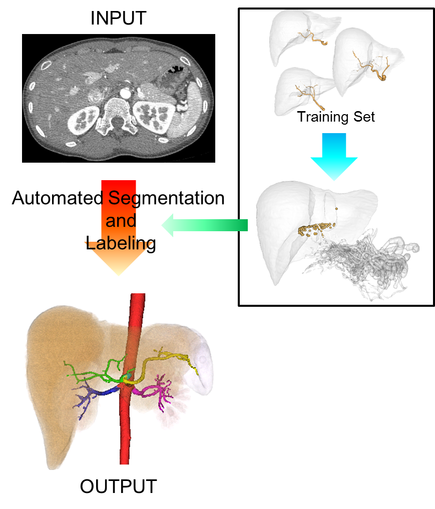
Understanding of abdominal vascular structures plays an important role in preoperative diagnosis, treatment planning, and intraoperative navigation. Our research focuses on automatic vessel structure recognition (vessel extraction and anatomical name mapping), which is useful for understanding vascular structures. We are developing a method to recognize vessels with complex three-dimensional structures and large inter-patient variability. Yuki Suzuki, Toshiyuki Okada, Masatoshi Hori, Futoshi Yokota, Marius George Linguraru, Noriyuki Tomiyama, Yoshinobu Sato, “Automated Segmentation and Anatomical Labeling of Abdominal Arteries Based on Multi-organ Segmentation from Contrast-Enhanced CT Data,” MICCAI 2012, Workshop on Clinical Image-based Procedures: From Planning to Intervention, LNSC, Vol. 7761, pp. 67-74 2013
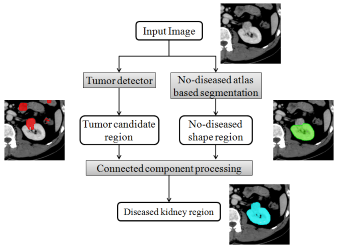
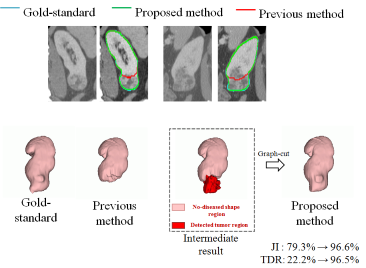
In this study, we propose a method for automatically extracting diseased kidneys from CT images. Although several methods have been proposed for automatic extraction of kidney regions from CT images, none of them has focused on diseased kidneys. Automatic extraction of diseased kidneys is important to support diagnosis and treatment. Tumors in the kidney have large variations in location and size, making statistical atlas methods unsuitable. Therefore, we used a detector that learned tumor image features by machine learning to detect tumors, and combined it with statistical atlas-based extraction of normal kidney regions to automatically extract the entire diseased kidney region. In our experiments, we evaluated 79 kidneys from 40 patients and found that the Jaccard index improved by about 4 points on average for all kidneys, and by about 7 points for affected kidneys only. From the experimental results, we believe that the proposed method shows a certain level of success as a method for extracting the entire tumor area. 福田紀生, 中本将彦, 岡田俊之, 小路直, 浮村理, GILL Inderbir S., 堀雅敏, 富山憲幸, 佐藤嘉伸, "腫瘍を有する腎臓の造影CT画像からの自動セグメンテーション", 第32回日本医用画像工学会大会, 東京, 2013年 7月.
Under construction.
Under construction.
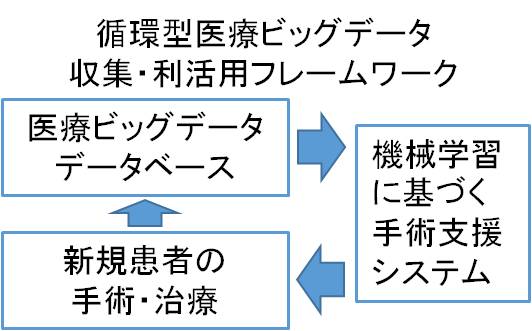
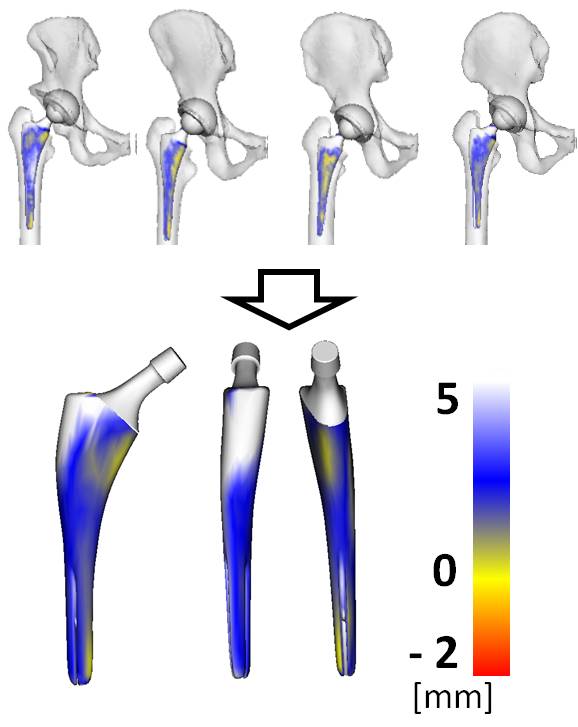
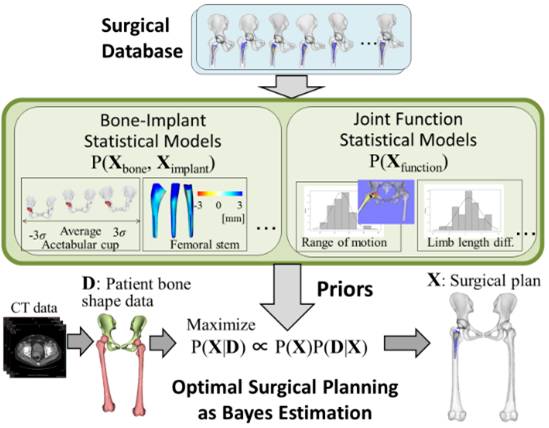
Medical image data such as CT and MRI data, surgical plans prepared by surgeons before surgery, and postoperative progress evaluations are usually stored in hospital databases after surgery or treatment is completed, and are rarely reused. As a way to effectively utilize the vast amount of medical data (medical big data) stored in hospitals, our laboratory is researching a system to apply information obtained through statistical learning from medical big data to surgical support (for details of this system, please refer to the "Surgical Support System" section). This system, which will benefit both patients and doctors, will enable the collection of more data as the importance of medical big data is widely recognized by society. In addition, the increase in training data will contribute to the improvement of the system's performance, thus creating a cyclical framework that has a synergistic effect of improving data collection and surgical safety. Japan Science and Technology Agency's Strategic Basic Research Program "PRESTO" (Research Area: Creation and Systematization of Next-Generation Fundamental Technologies for Integrated Utilization of Big Data) Project Title: Circulatory surgery support by integrating statistical learning and biological simulation
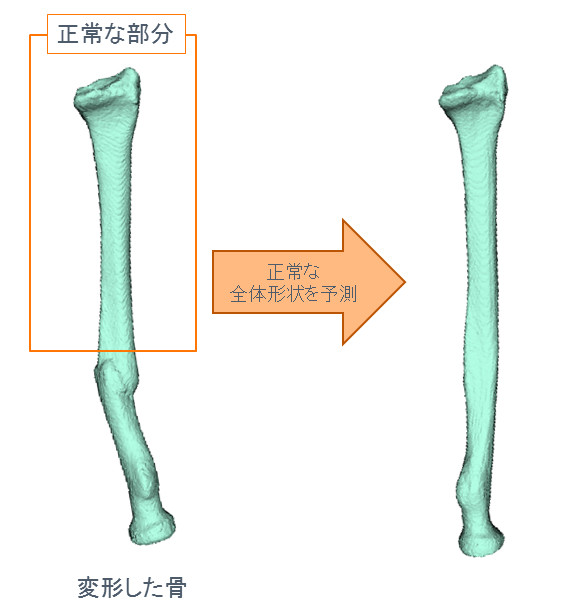
Methods of deformity correction targeting the healthy contralateral side using 3D CT images are becoming popular, but they are not applicable to bilateral deformities. Therefore, we are attempting to use statistical learning of normal bone shape in advance to predict the normal overall shape from the healthy part of the deformed bone, and to use this for surgical support.
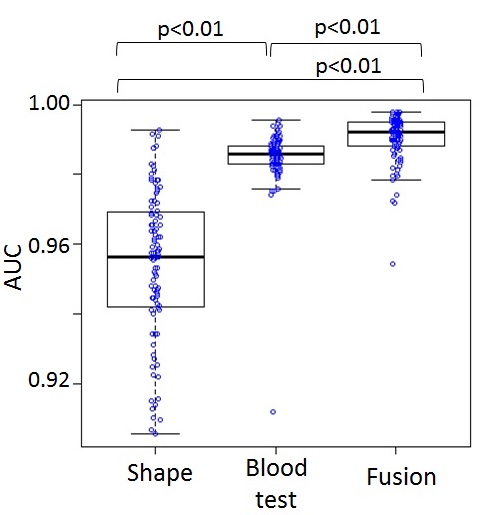
Although research on diagnostic support using medical images has been widely conducted, it will be important to integrate imaging information with other medical information to improve diagnostic accuracy in the future. Liver biopsy, which is currently used in clinical practice to confirm the diagnosis of liver fibrosis, is an invasive technique, and non-invasive methods are being investigated. Previous studies have reported methods for classifying liver fibrosis based on single pieces of information such as blood test information and liver morphology information obtained from CT images. In this study, we aim to integrate blood test information and morphological information to improve the accuracy of classification by integrating test and image information. A support vector machine was constructed by combining morphological and hematological information to classify liver fibrosis. 100 patterns of 3-fold cross-validation were tested and the area under the ROC curve (ROC) was evaluated. We confirmed that AUC was improved by integration. However, we also confirmed that there are cases that are difficult to classify by either blood test or morphology information. We plan to further integrate texture and stiffness information obtained from MRI and MR elastography to estimate fibrosis stage as well as presence/absence. 政木勇人,横田太,大竹義人,堀雅敏,岡田俊之,富山憲幸,佐藤嘉伸,"肝線維化症の診断支援に向けた画像情報と検査情報の統合法の検討 -血液検査情報に基づく診断への形態情報の統合-," 電子情報通信学会技術研究報告,医用画像,Vol.114,pp.59-62,2015年3月
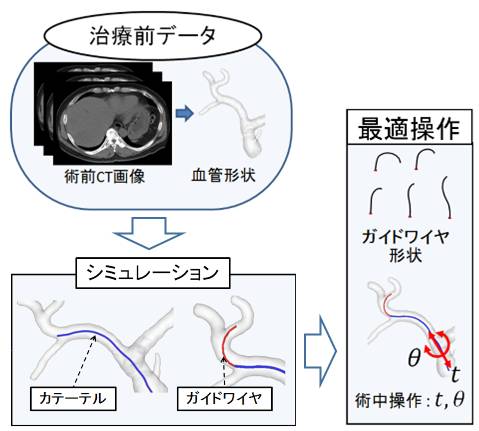
Optimization of catheter operation is performed based on the patient's unique vascular geometry obtained from 3D medical images (CT images) of the inside of the human body. We optimize intraoperative operations by statistically modeling the shape of surgical instruments used in the procedure and simulating the passage of the instruments through the blood vessels.
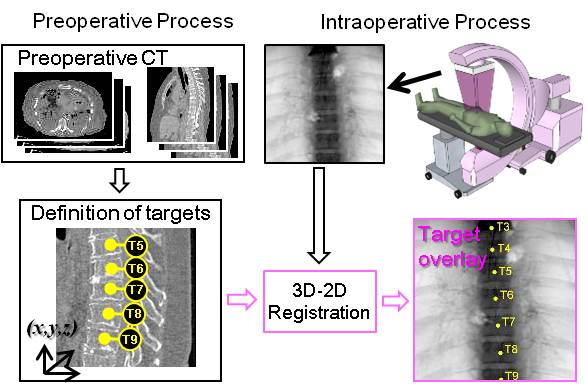
In spine surgery, X-ray images are used to locate the vertebrae to be operated on before surgery begins, and since all vertebrae look very similar in the 2D projection image, a process called level counting is performed, in which the vertebrae are counted in order from the most characteristic part, such as the neck or pelvis, to the target vertebrae. However, mistakes can occur in this process, and it has been reported that one out of every 3,000 spine surgeries is a strong-level surgery, which is a surgical error. We are researching a system that uses 2D-3D registration to precisely identify the target vertebrae intraoperatively by superimposing the positional information of the target area identified on the 3D image before surgery on the 2D projected image during surgery. This system received the 2013 Spine Technology Award (sponsored by Orthopaedics This Week). Otake, Y., A. S. Wang, A. Uneri, G. Kleinszig, S. Vogt, N. Aygun, S.-f. L. Lo, J.-P. Wolinsky, Z. L. Gokaslan and J. H. Siewerdsen (2015). "3D–2D registration in mobile radiographs: algorithm development and preliminary clinical evaluation." Physics in Medicine and Biology 60(5): 2075. Otake, Y., A. S. Wang, J. Webster Stayman, A. Uneri, G. Kleinszig, S. Vogt, A. J. Khanna, Z. L. Gokaslan and J. H. Siewerdsen (2013). "Robust 3D-2D image registration: application to spine interventions and vertebral labeling in the presence of anatomical deformation." Phys Med Biol 58(23): 8535-8553. Liu, W., Y. Otake, M. Azizian, O. Wagner, J. Sorger, M. Armand and R. Taylor (2014). "2D–3D radiograph to cone-beam computed tomography (CBCT) registration for C-arm image-guided robotic surgery." International Journal of Computer Assisted Radiology and Surgery: 1-14. Armiger, R. S., Y. Otake, A. S. Iwaskiw, A. C. Wickwire, K. A. Ott, L. M. Voo, M. Armand and A. C. Merkle (2014). Biomechanical Response of Blast Loading to the Head Using 2D-3D Cineradiographic Registration. Mechanics of Biological Systems and Materials, Volume 4. F. Barthelat, P. Zavattieri, C. S. Korach, B. C. Prorok and K. J. Grande-Allen, Springer International Publishing: 127-134.
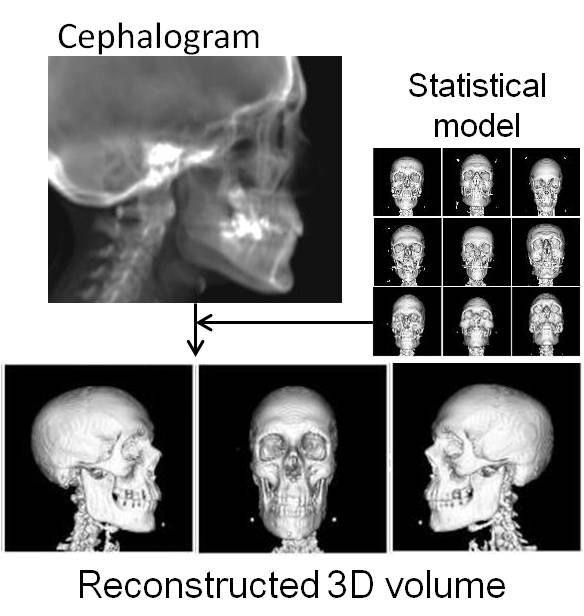
X-ray projection images are used in various clinical situations, such as head X-ray cephalometric images for dental treatment, to evaluate the extent of disease, and to confirm the success or failure of surgical procedures. Although it is difficult to precisely measure the three-dimensional position and shape of a target structure from a two-dimensional projection image, skilled physicians can envision a rough three-dimensional structure from this two-dimensional image alone. This is thought to be due to their knowledge of the skeletal shapes of many patients in the past. We are researching a method that uses machine learning to reproduce the estimation process of a skilled physician, and to reconstruct the 3D structure with an accuracy that exceeds that of a skilled physician. That is, we use statistical learning from a large number of previous 3D images of subjects to estimate the most plausible 3D shape from a unidirectional (or bidirectional) X-ray projection. This enables not only highly accurate 3D measurements from minimally invasive 2D images, but also various 3D analyses such as surgical navigation and post-operative motion analysis.
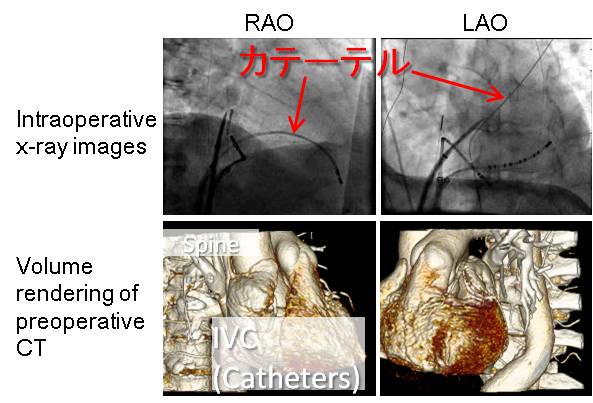
In cardiac catheterization, a thin tube-like catheter inserted from the base of the thigh is guided into the lumen of the heart using X-ray images from two directions called RAO (Right Anterior Oblique) and LAO (Left Anterior Oblique) to guide the catheter to the desired location in the beating heart. The catheter is inserted at the base of the thigh and guided through the lumen of the heart. The catheter is guided through a lumen in the beating heart, and the surgeon estimates the three-dimensional position of the catheter tip in relation to the heart based on the feel of the catheter in his or her hand, the slight movement of the cardiac limbus on the image, and the patient's disease level, age, and gender. To assist in this extremely difficult procedure, we are working on a system that can obtain information on the three-dimensional position of the heart and its motion from a bi-directional X-ray image by making maximum use of prior knowledge obtained from cardiac dynamic simulations and statistical atlases.
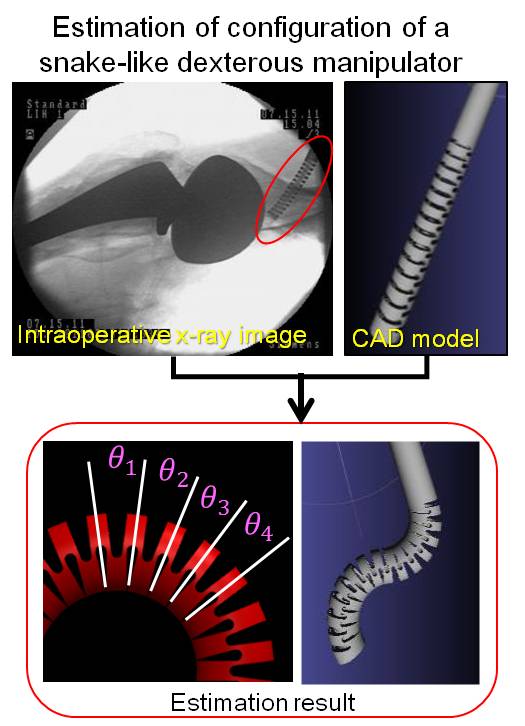
In recent years, surgical robots such as da Vinci have become popular. However, current surgical robots have only one joint at the tip (slave arm) that touches the patient, limiting the number of manipulatable objects. Therefore, the Snake-type robotic arm (left figure), which has many joints, is being actively studied. However, on the other hand, it is difficult to control the robot's shape (angles of all joints) with high precision because of its large deformation in response to external force. To solve this problem, we are developing a system that enables high-precision control throughout the entire surgery by using X-ray projection images to measure the shape of the robot inside the body during the surgery, and feeding this information back to the control system for repeated calibration. Otake, Y., R. J. Murphy, M. D. Kutzer, R. H. Taylor and M. Armand (2014). Piecewise-rigid 2D-3D registration for pose estimation of snake-like manipulator using an intraoperative x-ray projection. Medical Imaging 2014: Image-Guided Procedures, Robotic Interventions, and Modeling, Proc SPIE.
Arthroscopic surgery is less burdensome for the patient because the surgical wound is small, but the surgeon's burden is great because of the narrow field of view. Therefore, a surgical support system using augmented reality has been developed. Because arthroscopes are oblique endoscopes and have large image distortion, conventional camera models cannot properly display superimposed images. Therefore, we proposed a new camera model suitable for arthroscopes. In the conventional method, the superimposition error increases as the rotation angle of the lens barrel increases, but in the proposed method, the superimposition error does not change significantly as the rotation angle increases. Norio Fukuda, Masahiko Nakamoto, Toshiyuki Okada, Yen-Wei Chen and Yoshinobu Sato, “Comparison of accuracy on camera calibration method with distortion correction for oblique-viewing endoscope for computer assisted endoscopic surgery,” IEICE Tech. Rep., vol. 109, no. 407, MI2009-91, pp. 87-92, Jan. 2010.
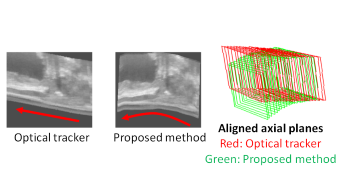
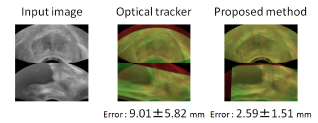
In the local treatment of the prostate, accurate positioning of the lesion is important, and a system that measures the position of the ultrasound probe using a three-dimensional position sensor and assists puncture placement has been developed for precise recording of the biopsy position and accurate guidance of the probe to the lesion. However, the use of position sensors may hinder smooth treatment in terms of installation cost, time and labor required for preoperative installation, and limited range of motion due to sensor measurement conditions. Therefore, we have proposed a new method to support puncture without using a position sensor by replacing the position and posture measurement with position and posture estimation based on image alignment in existing systems. Since the proposed method is based on image alignment, it can be expected to follow the movement and deformation of internal tissues during the operation, which is difficult to achieve using only a position sensor. We will conduct experiments using the Cadaver, which is capable of capturing images close to the actual images of the patient, to investigate the feasibility of the proposed method for clinical use. Norio Fukuda, Masahiko Nakamoto, Toshiyuki Okada, Yoshito Otake, Sunao Shoji, Japan, Osamu Ukimura, Inderbier S. Gill, USA, Yoshinobu Sato, "Cadaver evaluation of image-based tracking using biplane transrectal ultrasound probe for focal prostate therapy." the 2015 Joint Conference of the International Workshop on Advanced Image Technology (IWAIT) and the International Forum on Medical Imaging in Asia (IFMIA), Tainan, Jan. 2015.
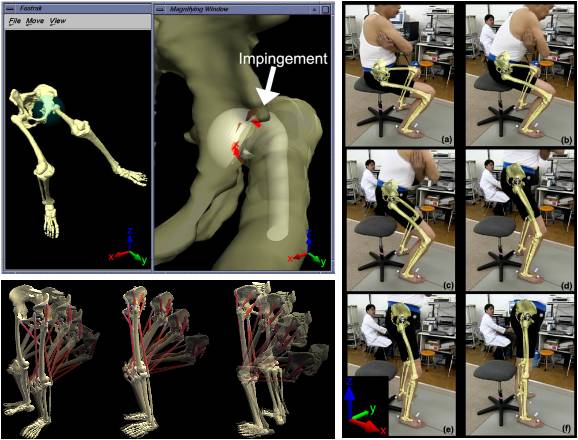
Under construction. Otake, Y., N. Suzuki, A. Hattori, K. Hagio, N. Sugano, K. Yonenobu and T. Ochi (2005). "Four-dimensional model of the lower extremity after total hip arthroplasty." J Biomech 38(12): 2397-2405. Otake, Y., N. Suzuki, A. Hattori, H. Miki, M. Yamamura, K. Yonenobu, T. Ochi and N. Sugano (2007). "System for intraoperative evaluation of soft-tissue-generated forces during total hip arthroplasty by measurement of the pressure distribution in artificial joints." Computer Aided Surgery 12(1): 53-59.
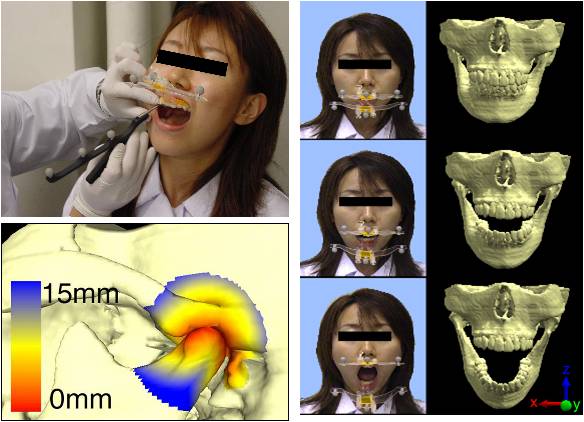
Under construction. Otake, Y., N. Suzuki, A. Hattori, Y. Shigeta, T. Ogawa, S. Fukushima, K. Kobayashi and A. Uchiyama (2006). "Real‐time mandibular movement analysis system using four‐dimensional cranial bone model." Systems and Computers in Japan 37(8): 1-12.